
Ever felt like the room is spinning when you haven't moved at all? Or maybe you just felt light-headed enough to grab a chair? Most people lump these sensations together under one label: dizziness. But in the world of medicine, the distinction matters deeply. Confusing the two can lead to years of wasted treatments-like taking anxiety meds for an inner ear crystal problem. Getting the diagnosis right isn't just about comfort; it’s about safety, because some causes are benign while others signal serious brain health issues.
Understanding the mechanics behind these symptoms is the first step toward relief. While Vertigo is an illusion of movement where the environment spins around you. It is Rotational Dizziness, specifically tied to inner ear dysfunction. Dizziness, on the other hand, is often vague, covering everything from lightheadedness to unsteadiness. Research indicates that about 20-30% of patients presenting with dizziness actually have vertigo. Yet, misdiagnosis remains rampant. A look at clinical data from King Edward VII Hospital shows that correctly diagnosing Benign Paroxysmal Positional Vertigo (BPPV) results in an 85% resolution rate, whereas treating it as general dizziness yields only a 45% success rate. That gap represents months of unnecessary suffering.
Anatomy of the Problem: Where Sensations Begin
To understand why you feel this way, we need to look at the machinery inside your head. Your sense of balance doesn't live in your brain alone; it relies heavily on the Vestibular System is the sensory system responsible for providing sense of balance and spatial orientation. It includes the Inner Ear and connects to the Brainstem. This system uses fluid-filled loops called semicircular canals to detect rotation and otolith organs to track linear movement. When these parts send mismatched signals to your brain, you get a conflict known as sensory dissonance.
The timing is crucial here. Normally, the vestibular system transmits head movement data to the brain with a latency of just 100-200 milliseconds. If that signal gets delayed or scrambled, your brain creates the illusion of motion. This disruption is the hallmark of true vertigo. In contrast, general dizziness often stems from cardiovascular changes, like orthostatic hypotension. According to MyHealth Alberta guidelines, a drop in systolic blood pressure of 20 mmHg or more upon standing can cause lightheadedness without any sensation of spinning. Knowing whether you feel faint or feel like the floor is moving dictates which doctor you see-a cardiologist or an ENT specialist.
Common Triggers for Rotational Sensations
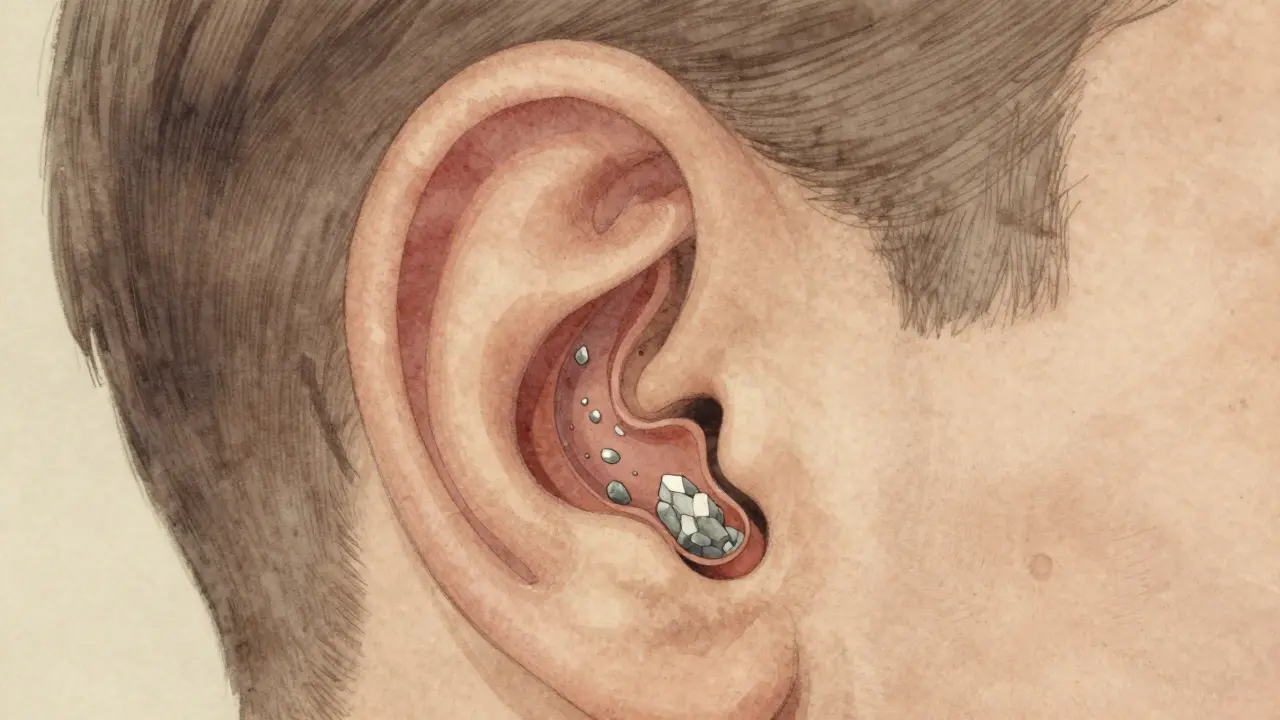
Not all spinning feels the same. Peripheral vestibular disorders are the most frequent culprits for true vertigo. BPPV is Benign Paroxysmal Positional Vertigo caused by displaced otolith crystals. It affects approximately 20-30% of vertigo cases globally. Think of it like gravel in a lock mechanism. Tiny calcium carbonate crystals, normally stuck in the otolith organs, break loose and float into the semicircular canals. When you tilt your head, these particles shift, dragging fluid with them and triggering a false alarm that you are spinning wildly. Dr. Timothy Hain from Northwestern University notes that BPPV is the single most common vestibular condition, impacting roughly 2.4% of the population annually.
Another well-known cause is Ménière's Disease is a chronic disorder affecting the inner ear causing episodes of vertigo. It impacts about 615,000 Americans.This condition involves a buildup of fluid pressure (endolymphatic hydrops). Unlike the quick bursts of BPPV, Ménière's attacks last hours. Patients typically experience a triad of symptoms: vertigo, tinnitus (ringing in the ears), and fluctuating hearing loss. Then there is vestibular neuritis, usually triggered by a virus inflaming the nerve connecting the ear to the brain. This type of inflammation can cause severe nausea and continuous imbalance for days until the body adapts.
| Condition | Primary Symptom | Duration | Hearing Loss? |
|---|---|---|---|
| BPPV | Positional Spinning | Seconds to Minutes | No |
| Ménière's | Severe Rotation + Noise | 20 Mins to Days | Yes (Fluctuating) |
| Vestibular Neuritis | Continuous Imbalance | Days to Weeks | Rarely |
When the Brain Gets Involved: Neurological Causes
Sometimes the issue isn't in the ear, but in how the brain processes the signals. Central vertigo originates in the brainstem or cerebellum. These cases are rarer, accounting for only 5-10% of vertigo cases according to Dr. David Zee of Johns Hopkins, but they carry higher risk. The main concern here is distinguishing a minor migraine from a stroke. Cerebellar strokes can mimic vertigo perfectly. Doctors look for "red flags" to differentiate them. If you have difficulty speaking (dysarthria), double vision (diplopia), or cannot walk straight without staggering significantly (ataxia), the problem is likely central.
Vestibular Migraine is A neurological condition combining headache and dizziness. It accounts for 7-10% of vertigo cases.This is a particularly tricky diagnosis. Up to 30% of these cases are initially misdiagnosed as sinusitis or anxiety. The headaches might not even hurt during the dizzy spell; sometimes it's just the spinning sensation that links back to migraine biology. Dr. Michael Teixido notes that this condition affects about 1% of the general population but is a leading cause of recurrent non-BPPV vertigo. Identifying this correctly saves patients from invasive surgeries meant for ear problems, as migraine management requires different lifestyle adjustments and medication classes.
Getting the Right Diagnosis
Finding out what's wrong requires a systematic approach. Primary care doctors struggle here; surveys indicate only 12% feel "very confident" diagnosing complex vertigo cases. Specialized testing is often needed. One gold standard tool is videonystagmography (VNG). This test tracks eye movements to assess function. It has a 95% sensitivity for peripheral disorders, meaning it catches almost every case of inner ear damage. For BPPV, doctors use physical maneuvers like the Dix-Hallpike test to provoke symptoms. If the test triggers nystagmus (eye twitching) after a specific head tilt, BPPV is confirmed immediately.
In urgent settings, doctors rely on the HINTS exam (Head Impulse, Nystagmus, Test of Skew). This bedside assessment helps rule out posterior circulation strokes, which account for 2-3% of vertigo presentations but require immediate intervention. Dr. Kevin Kerber highlights a concerning statistic: older adults often have multifactorial causes, with 50% having more than one issue complicating the picture. Consequently, patient history is king. If your dizziness started suddenly and never stops, it might be neuritis. If it happens only when rolling over in bed, it's almost certainly BPPV. Accuracy improves dramatically when symptoms are categorized precisely.
Treatment Paths and Recovery
Once the culprit is identified, effective treatments exist for nearly every condition. For BPPV, the Epley Maneuver is A specific repositioning procedure to fix BPPV. It has 80-90% efficacy rates. This procedure takes mere minutes. A therapist moves your head through a sequence of positions designed to guide those loose crystals back to their proper chamber. Most patients feel better after just one visit. Contrast this with vestibular rehabilitation therapy (VRT) used for neuritis or PPDD (Persistent Postural-Perceptual Dizziness). VRT requires commitment. It involves customized exercises progressing from static balance to dynamic activities. Studies from UCHealth show significant improvement after 6-8 weeks of consistent practice. Compliance is key; 35% of patients stop early because the exercises temporarily make them feel worse before getting better.
For medical management, steroids and antivirals help acute vestibular neuritis in the short term. Long-term, preventing falls is priority number one. The market reflects this growing need. As of late 2023, specialized vestibular clinics are now present in 78% of academic medical centers compared to just 32% of community hospitals a decade ago. Newer technologies like the FDA-approved VRT-1 device aim to gamify recovery, making home therapy more engaging. Ultimately, the path to feeling grounded again exists. It starts with recognizing that not all dizziness is created equal and seeking the expert who can tell the difference.
How do I know if my dizziness is serious?
If your dizziness comes with severe headache, trouble speaking, weakness on one side, or double vision, seek emergency care immediately. These could be signs of a stroke rather than a simple inner ear issue.
Can anxiety cause real vertigo?
Anxiety can worsen the sensation of imbalance, particularly a condition called PPDD. However, pure spinning vertigo is rarely caused solely by anxiety. Misdiagnosis of vestibular issues as anxiety is common, happening in over 30% of vestibular migraine cases.
How long does BPPV last?
Without treatment, BPPV can wax and wane for months. With a successful Epley maneuver, many patients experience complete resolution within one to three sessions.
Is vertigo permanent?
Chronic conditions like Ménière's disease may persist, but symptom frequency usually decreases over time. Many other causes, like viral neuritis or BPPV, resolve fully with the vestibular system compensating for the damage.
What tests are needed for diagnosis?
Basic assessments include the Dix-Hallpike maneuver. More advanced testing involves Videonystagmography (VNG) or MRI scans if central neurological causes are suspected. Blood work may also rule out metabolic factors.








Most people confuse these terms and end up wasting money on useless therapy.
The anatomy is clear and you just ignore basic physiology.
It takes actual medical training to distinguish these signals properly.
Ignoring the vestibular system leads to wasted years of treatment.
You clearly missed the point about the brainstem involvement.
Stop posting vague health theories without reading the data.
I spent so many months wondering why my house spun when I turned around.
Every specialist I visited gave me a different medication to try.
I felt terrible knowing they did not understand the root cause.
Finally one doctor sat down and explained how fluid moves in the ear.
She showed me diagrams of the tiny crystals causing the problem.
It turns out gravity played a much bigger role than I thought.
We performed the maneuver right there in the small clinic room.
My relief was immediate after she finished moving my head.
I cried because I finally understood what had been wrong all along.
Now I tell everyone to check their inner ear before panic sets in.
Misdiagnosis really damages your spirit when nothing gets better.
Reading this post validates everything I went through recently.
Medical experts should share this information with primary care staff.
It prevents so much unnecessary suffering for regular patients like me.
You do not have to live with fear of moving your neck.
Actually the public understanding varies quite a bit depending on education.
It helps to explain things simply for those searching for help.
Many people are scared to seek assistance from medical teams.
Providing clear definitions reduces confusion significantly for families involved.
We all benefit from knowing the warning signs exist early.
i know this feels scary sometimes but the body heals well often
doctors need to listen closer to patient descriptions of motion
maybe it is just the blood pressure changing things around
still glad we have better tests now than back then
You claim the doctor fixed it instantly which is unlikely in reality.
Recovery usually involves weeks of rehabilitation work.
Some sources suggest psychological factors are ignored heavily here.
Your experience sounds like a very specific case scenario only.
great summary of the differences between conditions
this info makes me feel less worried about upcoming visits
hope everyone finds the right specialist soon
You need to take action rather than waiting for worry.
Symptoms like stumbling indicate central nervous system issues.
Do not delay testing if the spinning feels continuous.
Immediate care prevents worse outcomes later on.
This information is widely known by professionals.
While simplified explanations aid understanding, clinical nuance remains essential.
The differentiation between peripheral and central causes dictates prognosis.
Further research into vestibular migraine pathways warrants attention.
Accurate categorization facilitates appropriate therapeutic interventions effectively.