
What Exactly Is Hyperpigmentation?
Hyperpigmentation isn’t one condition-it’s a symptom. Your skin makes too much melanin in certain spots, and those spots get darker. It’s not dangerous, but it can be frustrating, especially when it shows up on your face. Two of the most common causes are melasma and sun damage. They look similar, but they’re not the same. Mixing them up leads to the wrong treatment-and sometimes, worse pigmentation.
Melasma: More Than Just a Tan
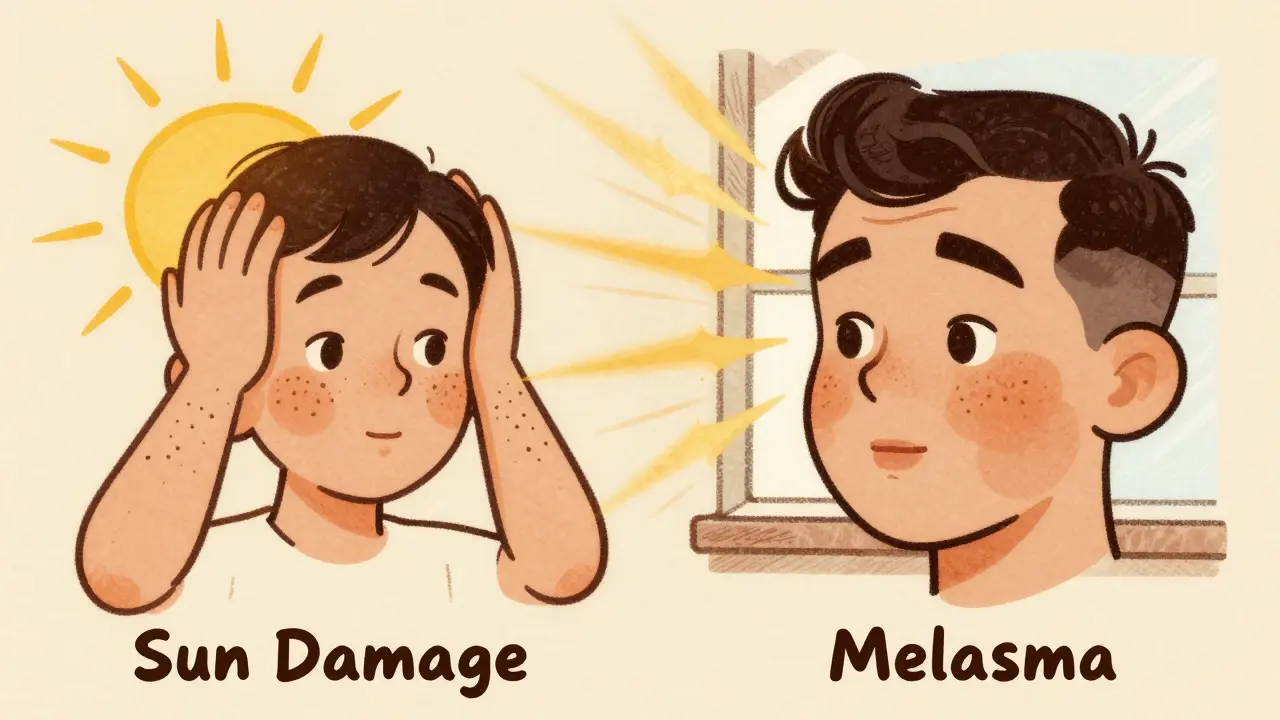
Melasma shows up as large, patchy brown or gray-brown areas, usually on the cheeks, forehead, nose, or upper lip. It’s not caused by one thing. Hormones play a big role. That’s why it’s so common in women during pregnancy (called the "mask of pregnancy"), on birth control, or during hormone therapy. It also affects women with medium to dark skin tones-Fitzpatrick types III to VI-much more often than lighter skin. Studies show Black, Asian, and Hispanic women are 3 to 5 times more likely to develop it than Caucasian women.
What makes melasma tricky is that it’s triggered by more than just UV light. Visible light from windows, screens, and even fluorescent bulbs can make it worse. Heat, too. That’s why a regular sunscreen isn’t enough. You need one with iron oxides-mineral sunscreens with zinc oxide and iron oxides block visible light. Without this, even the best topical treatments won’t hold.
Sun Damage: The Slow Burn of UV Exposure
Sun damage, or solar lentigines, looks different. These are small, well-defined spots-think freckles that got bigger. They show up on your face, hands, shoulders, and arms. They’re not hormonal. They’re purely from years of sun exposure. By age 60, about 90% of fair-skinned people have them. Unlike melasma, sun damage doesn’t spread in patches. It’s localized, and it responds well to treatment.
Here’s the key difference: melasma is reactive. It flares with heat, light, and hormones. Sun damage is cumulative. It’s like a tattoo your skin made over time. Treatments like IPL (intense pulsed light) work great on sun spots because they target the pigment directly. But if you use IPL on melasma, you risk making it worse. Heat activates melanocytes, and melasma is already overactive.
Topical Treatments That Actually Work
Not all creams are created equal. The most effective topical treatments target melanin production at different points. Here’s what dermatologists actually use:
- Hydroquinone (4%): This is the gold standard. It blocks the enzyme tyrosinase, which your skin uses to make melanin. Used alone, it helps about 30-40% of people. But when combined with tretinoin and a corticosteroid (a triple combo), success jumps to 50-70% in 12 weeks. Limit use to 3 months at a time. Longer use can cause ochronosis-a rare but permanent bluish-gray discoloration.
- Tretinoin (0.025%-0.1%): This vitamin A derivative speeds up skin cell turnover. It doesn’t lighten pigment directly. Instead, it pushes the darkened cells to the surface faster so they flake off. Used every other night, it boosts hydroquinone’s effect and prevents clogged pores.
- Vitamin C (10%-20% L-ascorbic acid): A powerful antioxidant. It doesn’t just prevent free radical damage. It also reduces existing oxidized melanin and blocks tyrosinase. Apply it every morning before sunscreen. It’s gentle, stable, and works well with other ingredients.
- Tranexamic acid (5%): Originally a blood thinner, it’s now used topically for melasma. It interrupts signals between skin cells and melanocytes. In clinical trials, it reduced melasma by 45% in 12 weeks with almost no irritation. It’s especially useful for people who can’t use hydroquinone.
- Niacinamide (5%): Reduces melanin transfer to skin cells. It’s mild, hydrating, and safe for long-term use. Great for maintenance after initial treatment.
Why Most People Fail at Treating Melasma
It’s not the products. It’s the routine. The biggest mistake? Inconsistent sun protection. Dermatologists say 70% of patients don’t use enough sunscreen. They apply less than a quarter-teaspoon for their face. And they forget to reapply every two hours-especially if they’re near windows or outside.
Another problem: expecting quick results. Melasma doesn’t vanish in a week. It takes 8 to 12 weeks just to see a change. And even then, you’re not done. Up to 95% of people see it come back within 6 months if they stop treatment. That’s why maintenance is non-negotiable. You need to keep using sunscreen and at least one lightening agent-like niacinamide or vitamin C-forever.
Laser and Light Therapies: When to Use Them
Laser treatments aren’t the first step for melasma. In fact, they’re often the last. Dermatologists won’t even consider them until the melanocytes are calmed down with 8 to 12 weeks of topical therapy. Why? Because lasers generate heat. And heat triggers melasma.
IPL works great for sun damage. It breaks up pigment in 1-2 sessions. But for melasma, the risk of rebound pigmentation is 30-40%. Chemical peels (like glycolic or salicylic acid) are safer. Done every 4-6 weeks, they improve results by 35-50% compared to topicals alone. But again, they’re only safe if your skin is stable.
For darker skin tones, lasers carry a higher risk of post-inflammatory hyperpigmentation (PIH). That’s why many dermatologists avoid them entirely for Fitzpatrick IV-VI skin unless they’re using very low-energy settings.
What’s New in 2026
The hyperpigmentation market is growing fast-projected to hit $22 billion by 2030. That’s because people are demanding better, safer options.
Hydroquinone is under review by the FDA. It might become available without a prescription, but with strict safety labeling. Meanwhile, non-hydroquinone options are rising fast. Cysteamine cream (10%) showed 60% improvement in melasma in recent trials with minimal side effects. Tranexamic acid pills are now being studied for oral use in stubborn cases.
Personalized treatment is coming. Dermatologists are starting to use skin analysis tools that map melanin patterns and genetic markers. In five years, your treatment may be based on your DNA-not just your skin tone.
What You Can Do Today
Start simple:
- Use a mineral sunscreen with zinc oxide and iron oxides every morning. Apply a quarter-teaspoon to your face and neck. Reapply every 2 hours if you’re outside.
- At night, alternate between 4% hydroquinone and 0.05% tretinoin every other night. If your skin gets irritated, start with 2-3 nights a week and build up.
- Use a vitamin C serum (15% L-ascorbic acid) every morning before sunscreen.
- Don’t skip the moisturizer. Dry skin worsens irritation and slows healing.
- See a dermatologist if you don’t see improvement in 12 weeks. They can add chemical peels or adjust your regimen.
And remember: hyperpigmentation isn’t a flaw. It’s your skin’s response to stress-hormones, sun, inflammation. Treat it like a chronic condition, not a quick fix. Consistency beats intensity every time.
Frequently Asked Questions
Can melasma go away on its own?
Sometimes, yes-but only if the trigger is removed. Melasma from pregnancy often fades after delivery. Melasma from birth control may improve if you switch methods. But if sun exposure continues, it won’t disappear. Most cases need active treatment and long-term sun protection to improve.
Is hydroquinone safe to use long-term?
No. Hydroquinone should be used for no more than 3 months at a time due to the risk of ochronosis-a rare but permanent darkening of the skin. After 3 months, switch to maintenance agents like niacinamide, tranexamic acid, or vitamin C. You can cycle hydroquinone on and off under a dermatologist’s guidance.
Why does my sunscreen still let my melasma get worse?
Most sunscreens only block UV rays. But melasma is also triggered by visible light and heat. You need a mineral sunscreen with iron oxides-these block visible light. Look for products labeled "broad-spectrum with iron oxide" or check the ingredients list. Zinc oxide alone isn’t enough.
Can I use retinol instead of tretinoin for melasma?
Retinol is weaker than tretinoin and may not be strong enough to speed up skin turnover effectively. Tretinoin (0.025%-0.1%) is prescription-strength and clinically proven to enhance pigment clearance when paired with hydroquinone. Over-the-counter retinol might help with texture, but it won’t deliver the same results for pigmentation.
How long does it take to see results from topical treatments?
Most people start seeing subtle lightening after 6-8 weeks. Noticeable improvement usually takes 12 weeks. Melasma responds slowly because melanin is deeply embedded. Patience and consistency are key. Stopping too early is the most common reason treatments fail.
Is melasma more common in certain skin tones?
Yes. Melasma affects women with medium to dark skin tones (Fitzpatrick III-VI) 3 to 5 times more often than those with lighter skin. This is because darker skin has more active melanocytes, which are more sensitive to hormonal and light triggers. It’s also why laser treatments carry higher risks for these skin types.
Can stress make hyperpigmentation worse?
Yes. Stress increases cortisol, which can stimulate melanocytes and worsen pigmentation. While it’s not a direct cause like hormones or sun, chronic stress can make melasma harder to treat. Managing stress through sleep, exercise, or mindfulness can support your skin’s healing process.




12 Comments
Write a comment